
See the long-term exploratory analyses for BAVENCIO
SEE 5+ YEARS OF EFFICACY FOR BAVENCIO1
Don't miss the real-world evidence below
- Primary and Long-Term Analyses
- Long-Term Exploratory Analyses
- Patient-Reported Outcomes
Strategize for Extended Overall Survival with BAVENCIO 1L Maintenance2,3
JAVELIN BLADDER 100 PRIMARY ANALYSIS: BAVENCIO + BSC demonstrated superior OS vs BSC alone2
Median follow-up: 19.6 months (95% CI: 18.0, 20.6) in the BAVENCIO + BSC arm; 19.2 months (95% CI: 17.4, 21.6) in the BSC-alone arm4
mOS of 21.4 MONTHS (95% CI: 18.9, 26.1) with BAVENCIO + BSC vs 14.3 MONTHS (95% CI: 12.9, 17.9) with BSC alone (n=350 in each arm); HR 0.69 (0.56, 0.86); 2-sided P valuea=0.0012
The pre-planned interim analysis was considered the primary analysis since the primary endpoint was met.3,5
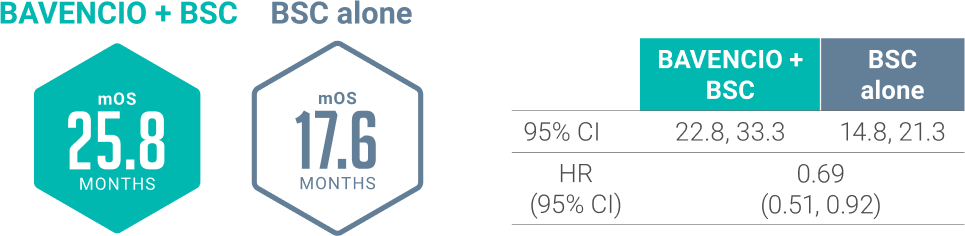
LONG-TERM ANALYSIS (3+ years): Consistent OS results were observed2
Median follow-up: 38.0 months (95% CI: 36.1, 40.5) in the BAVENCIO + BSC arm; 39.6 months (95% CI: 36.2, 41.7) in the BSC-alone arm3,5
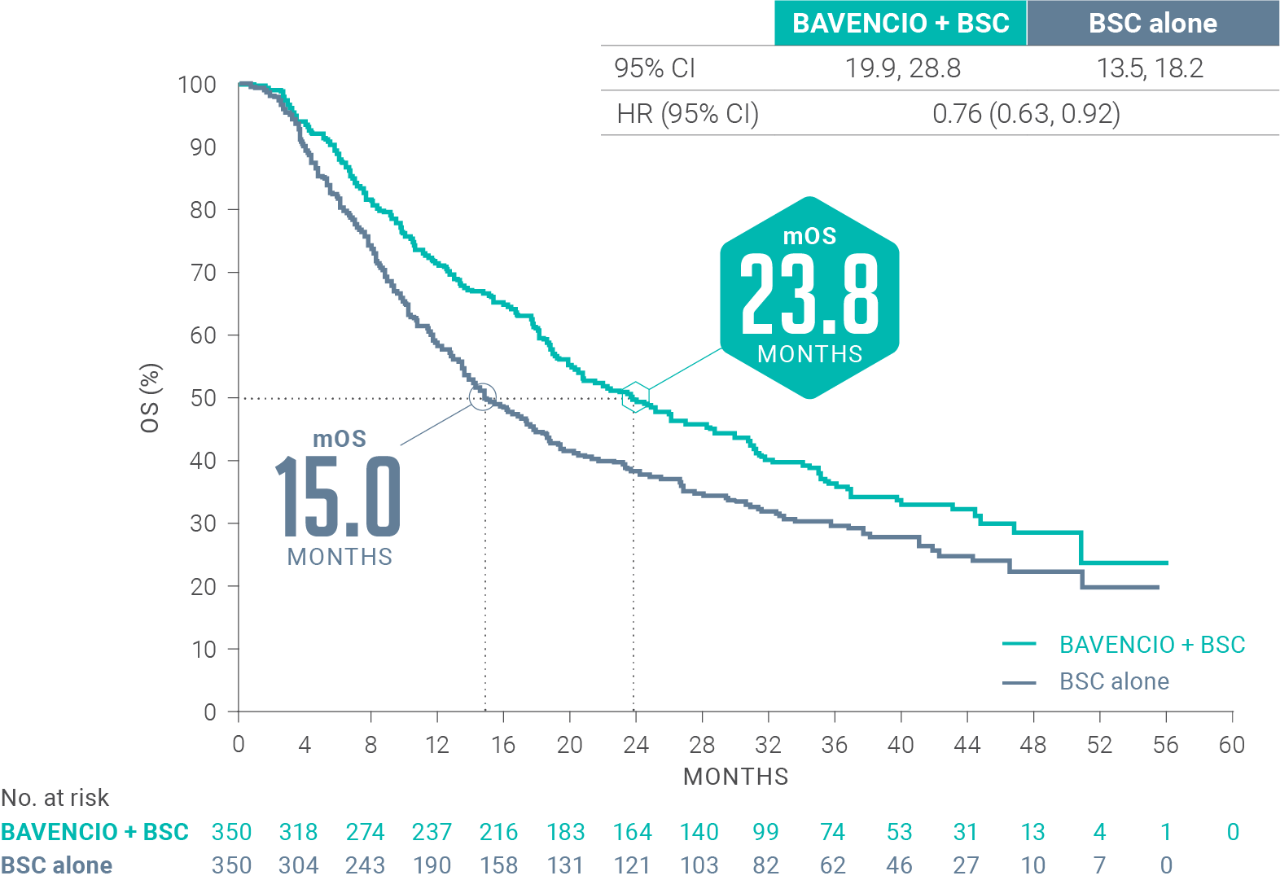
| BAVENCIO + BSC | BSC alone | |
|---|---|---|
| 95% Cl | 19.9, 28.8 | 13.5, 18.2 |
| HR (95% Cl) | 0.76 (0.63, 0.92) | |
Long-term OS results in PD-L1–positive patients2,b (n=358, 51% of patients): HR 0.69 (95% CI: 0.52, 0.90)
PD-L1–negative tumors2 (exploratory analysis; n=270, 39% of patients): OS HR 0.82 (95% CI: 0.62, 1.09)
While the long-term OS analysis was prespecified, no formal hypothesis testing was performed given OS was met in the interim analysis. No conclusions can be drawn from this analysis.
aP value based on stratified log-rank.6
bUsing the VENTANA PD-L1 (SP263) assay, PD-L1–positive status was defined as PD-L1 expression in ≥25% of tumor cells or in ≥25% or 100% of tumor-associated immune cells if the percentage of immune cells was >1% or ≤1%, respectively. If none of these criteria were met, PD-L1 status was considered negative.6
Additional exploratory data from the JAVELIN Bladder 100 trial
mOS of ~30 months from start of 1L platinum-containing chemotherapy5
LIMITATIONS:
These are exploratory, post hoc analyses of OS data, inclusive of platinum-containing chemotherapy (4-6 cycles), treatment-free interval (4-10 weeks, per trial protocol), randomized study treatment with BAVENCIO + BSC or BSC alone, and subsequent therapy. This analysis includes only patients who did not progress on first-line platinum-containing chemotherapy and subsequently enrolled in the JAVELIN Bladder 100 trial. Small patient numbers can be a limitation of subgroup analyses. Safety data are not available pre-randomization. No conclusions can be drawn from these OS analyses.

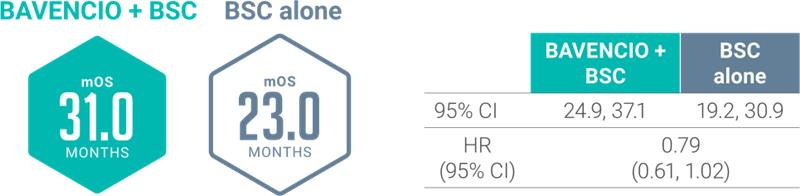
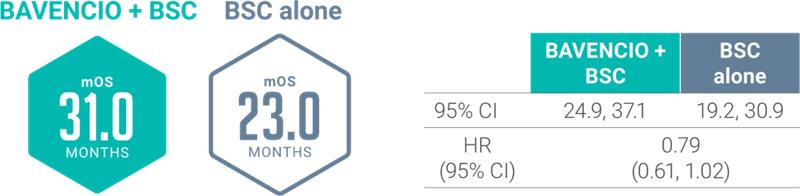
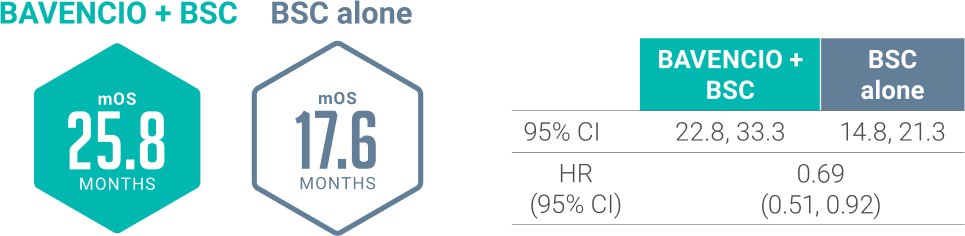
JB100 SUBGROUP ANALYSES showed mOS from the start of 1L platinum-containing chemotherapy regardless of type5
Prespecified Analysis: Cisplatin + Gemcitabinea
Tap to zoom in
Prespecified Analysis: Carboplatin + Gemcitabinea
Tap to zoom in
aStratified HR analyses are shown.7
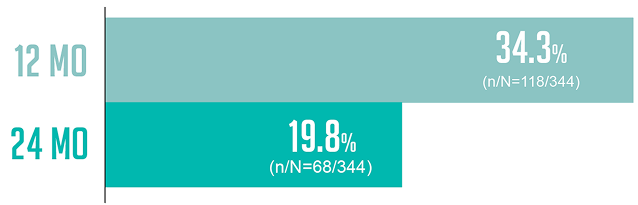
AN EXPLORATORY, POST HOC ANALYSIS: Duration of Treatment
An exploratory, post hoc analysis of patients who received BAVENCIO + BSC8
An exploratory, post hoc analysis of patients who received BAVENCIO + BSC8
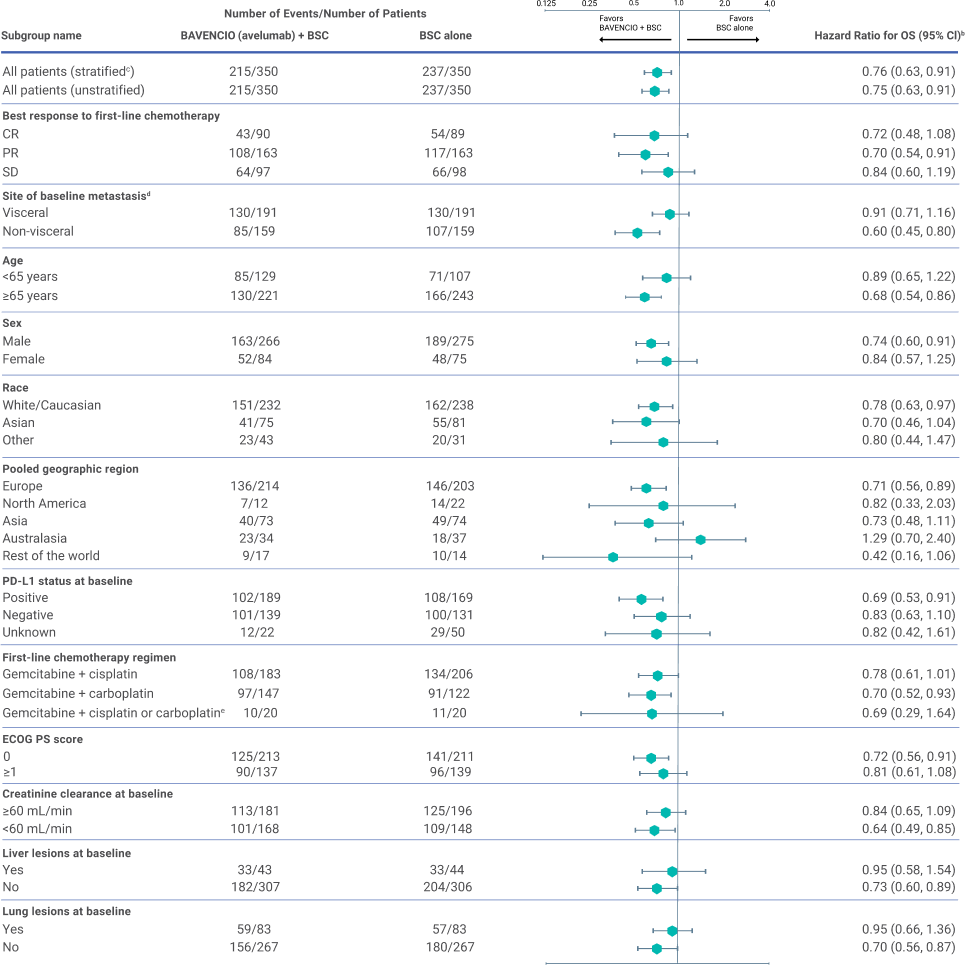
SUBGROUP ANALYSIS: OS analyses of prespecified subgroups in all randomized patients3
LIMITATIONS:
Small patient numbers can be a limitation of subgroup analyses. These results are presented for descriptive purposes and cannot be interpreted as a demonstration of efficacy in any particular subgroup. The results show the variability of the observed treatment effect over several subgroups. No adjustments were made for multiple comparisons in the subgroup analyses.
Hear from an expert on the efficacy outcomes from JAVELIN BLADDER 100 Trial
JAVELIN Bladder 100 Trial Efficacy Dr. Mehta
Patient-reported outcomes: A prespecified secondary endpoint from JB1009
- FBlSI-18 is a validated, bladder cancer–specific tool that measures symptoms and QOL in the past 7 days
- FBlSI-18 total score and subscales: In the mixed-effect model analysis, no significant differences were found between treatment arms in estimated mean scores or their corresponding subscales throughout all on-treatment cycles
FBlSI-18 analysis in the overall populationa

FBlSI-18 disease-related symptom subscalesa:
PHYSICAL (DRS-P)
pain, weight loss, urination, weakness, dizziness, meeting family needs, appetite, erection in males, and sleep
EMOTIONAL (DRS-E)
worrying about disease worsening, sadness
TREATMENT SIDE EFFECTS (TSE)
nausea, lack of energy, feeling ill, bowel control, bother of treatment side effects
FUNCTIONAL WELL-BEING (FWB)
ability to enjoy life, contentment with QOL
LIMITATIONS9:
- Open-label trial design and the limited number of patients providing data at later time points
- The limited number of patients at later cycles was prominent in the control arm, mainly due to progression events, which may limit the interpretation of longer-term PRO
- The FBlSI-18 instrument was validated in patients with bladder cancer, but some items may be less relevant for advanced disease in the maintenance setting
- All analyses were not adjusted for multiple testing, hindering their overall interpretation
- The methodology of this assessment does not allow conclusions based on these data
aRanges for each FBlSI-18 score: total, 0-72; DRS-P, 0-36; DRS-E, 0-8; TSE, 0-20; FWB, 0-8. Descriptive statistics were calculated for FBlSI-18 total score and subscales. Estimates of clinically important differences and changes for group comparisons: total, 3-6; DRS-P, 2-3; TSE, 1-2; and DRS-E and FWB, one each. Estimates of significant changes in individual patients: total, 3-9; DRS-P, 2-6; DRS-E, 1-3; TSE, 2-5; and FWB, 2-4.9
bNumber of patients who completed the baseline assessment and the assessment at the respective cycle. Data for on-treatment visits that had 10 or more patients in both arms are shown. For the BAVENCIO + BSC and BSC-alone arms, 333 and 330 patients responded to one or more items at baseline, respectively.9
Review sample patient profiles to find out if your patients with UC are also appropriate for 1L maintenance with BAVENCIO

1L=first line; BSC=best supportive care; CI=confidence interval; CR=complete response; ECOG PS=Eastern Cooperative Oncology Group Performance Status; FBISI=Functional Assessment of Cancer Therapy Bladder Symptom Index-18; HR=hazard ratio; JB100=JAVELIN Bladder 100 Trial; mOS=median overall survival; OS=overall survival; PD-L1=programmed death ligand-1; PRO=patient-reported outcome; QOL=quality of life; PR=partial response; SD=standard deviation; UC=urothelial carcinoma.
References: 1. PR Newswire. FDA Approves BAVENCIO as first-line maintenance treatment for patients with locally advanced or metastatic urothelial carcinoma. Press release. June 30, 2020. Accessed August 14, 2025. https://www.prnewswire.com/news-releases/fda-approves-bavencio-as-first-line-maintenance-treatment-for-patients-with-locally-advanced-or-metastatic-urothelial-carcinoma-301086396.html 2. Bavencio Prescribing Information. EMD Serono, Inc. 3. Powles T, Park SH, Caserta C, et al. Avelumab first-line maintenance for advanced urothelial carcinoma: results from the JAVELIN Bladder 100 Trial after ≥2 years of follow-up [supplementary appendix]. J Clin Oncol. 2023;41(19):3486-3492. 4. Grivas P, Park SH, Voog E, et al. Avelumab first-line maintenance therapy for advanced urothelial carcinoma: comprehensive clinical subgroup analyses from the JAVELIN Bladder 100 phase 3 trial. Eur Urol. 2023;84(1):95-108. 5. Data on file. EMD Serono, Inc., Boston, MA. 6. Powles T, Park SH, Voog E, et al. Avelumab maintenance therapy for advanced or metastatic urothelial carcinoma. N Engl J Med. 2020;383(13):1218-1230. 7. Sridhar SS, Powles T, Gupta S, et al. Avelumab first-line (1L) maintenance for advanced urothelial carcinoma: long-term follow-up from the JAVELIN Bladder 100 trial in subgroups defined by 1L chemotherapy regimen and analysis of overall survival from start of 1L chemotherapy. Abstract No. 508 presented at: 2023 ASCO Genitourinary Cancers Symposium; February 16-18, 2023; San Francisco, CA. 8. Grivas P, Park SH, Voog E, et al. Avelumab first-line maintenance in advanced urothelial carcinoma: conditional survival and long-term safety in patients treated for ≥1 or ≥2 years in JAVELIN Bladder 100. Poster #1975P presented at: European Society for Medical Oncology Congress 2024; September 13-17, 2024; Barcelona, Spain. 9. Grivas P, Kopyltsov E, Su P-J, et al. Patient-reported outcomes from JAVELIN Bladder 100: avelumab first-line maintenance plus best supportive care versus best supportive care alone for advanced urothelial carcinoma. Eur Urol. 2023;83(4):320-328.
INDICATIONS & IMPORTANT SAFETY INFORMATION
INDICATIONS
BAVENCIO® (avelumab) is indicated for:
- The maintenance treatment of patients with locally advanced or metastatic urothelial carcinoma (UC) that has not progressed with first-line platinum-containing chemotherapy
- The treatment of patients with locally advanced or metastatic UC who have disease progression during or following platinum-containing chemotherapy or have disease progression within 12 months of neoadjuvant or adjuvant treatment with platinum-containing chemotherapy
IMPORTANT SAFETY INFORMATION
IMPORTANT SAFETY INFORMATION
BAVENCIO can cause severe and fatal immune-mediated adverse reactions in any organ system or tissue and at any time after starting treatment with a PD-1/PD-L1 blocking antibody, including after discontinuation of treatment.
Early identification and management of immune-mediated adverse reactions are essential to ensure safe use of PD-1/PD-L1 blocking antibodies. Monitor patients closely for symptoms and signs that may be clinical manifestations of underlying immune-mediated adverse reactions. Evaluate liver enzymes, creatinine, and thyroid function at baseline and periodically during treatment. In cases of suspected immune-mediated adverse reactions, initiate appropriate workup to exclude alternative etiologies, including infection. Institute medical management promptly, including specialty consultation as appropriate.
No dose reduction for BAVENCIO is recommended. For immune-mediated adverse reactions, withhold or permanently discontinue BAVENCIO depending on severity. In general, withhold BAVENCIO for severe (Grade 3) immune-mediated adverse reactions. Permanently discontinue BAVENCIO for life-threatening (Grade 4) immune-mediated adverse reactions, recurrent severe (Grade 3) immune-mediated reactions that require systemic immunosuppressive treatment, or an inability to reduce corticosteroid dose to 10 mg or less of prednisone or equivalent per day within 12 weeks of initiating corticosteroids. In general, if BAVENCIO requires interruption or discontinuation, administer systemic corticosteroid therapy (1 to 2 mg/kg/day prednisone or equivalent) until improvement to Grade 1 or less. Upon improvement to Grade 1 or less, initiate corticosteroid taper and continue to taper over at least 1 month. Consider administration of other systemic immunosuppressants in patients whose immune-mediated adverse reactions are not controlled with corticosteroid therapy. Toxicity management guidelines for adverse reactions that do not necessarily require systemic corticosteroids (eg, endocrinopathies and dermatologic reactions) are discussed in subsequent sections.
BAVENCIO can cause immune-mediated pneumonitis. Withhold BAVENCIO for Grade 2, and permanently discontinue for Grade 3 or Grade 4 pneumonitis. Immune-mediated pneumonitis occurred in 1.1% (21/1854) of patients, including fatal (0.1%), Grade 4 (0.1%), Grade 3 (0.3%), and Grade 2 (0.6%) adverse reactions. Systemic corticosteroids were required in all (21/21) patients with pneumonitis.
BAVENCIO can cause immune-mediated colitis. The primary component of immune-mediated colitis consisted of diarrhea. Cytomegalovirus infection/reactivation has been reported in patients with corticosteroid-refractory immune-mediated colitis. In cases of corticosteroid-refractory colitis, consider repeating infectious workup to exclude alternative etiologies. Withhold BAVENCIO for Grade 2 or Grade 3, and permanently discontinue for Grade 4 colitis. Immune-mediated colitis occurred in 1.5% (27/1854) of patients, including Grade 3 (0.4%) and Grade 2 (0.8%) adverse reactions. Systemic corticosteroids were required in all (27/27) patients with colitis.
BAVENCIO can cause hepatotoxicity and immune-mediated hepatitis. Withhold or permanently discontinue BAVENCIO based on tumor involvement of the liver and severity of aspartate aminotransferase (AST), alanine aminotransferase (ALT), or total bilirubin elevation. Immune-mediated hepatitis occurred with BAVENCIO as a single agent in 1.1% (20/1854) of patients, including fatal (0.1%), Grade 3 (0.8%), and Grade 2 (0.2%) adverse reactions. Systemic corticosteroids were required in all (20/20) patients with hepatitis.
BAVENCIO can cause primary or secondary immune-mediated adrenal insufficiency. For Grade 2 or higher adrenal insufficiency, initiate symptomatic treatment, including hormone replacement, as clinically indicated. Withhold BAVENCIO for Grade 3 or Grade 4 endocrinopathies until clinically stable or permanently discontinue depending on severity. Immune-mediated adrenal insufficiency occurred in 0.6% (11/1854) of patients, including Grade 3 (0.1%) and Grade 2 (0.4%) adverse reactions. Systemic corticosteroids were required in all (11/11) patients with adrenal insufficiency.
BAVENCIO can cause immune-mediated hypophysitis. Hypophysitis can present with acute symptoms associated with mass effect such as headache, photophobia, or visual field defects. Hypophysitis can cause hypopituitarism. Initiate hormone replacement, as clinically indicated. Withhold BAVENCIO for Grade 3 or Grade 4 endocrinopathies until clinically stable or permanently discontinue depending on severity. Immune-mediated pituitary disorders occurred in 0.1% (1/1854) of patients, which was a Grade 2 (0.1%) adverse reaction.
BAVENCIO can cause immune-mediated thyroid disorders. Thyroiditis can present with or without endocrinopathy. Hypothyroidism can follow hyperthyroidism. Initiate hormone replacement for hypothyroidism or institute medical management of hyperthyroidism, as clinically indicated. Withhold BAVENCIO for Grade 3 or Grade 4 endocrinopathies until clinically stable or permanently discontinue depending on severity. Thyroiditis occurred in 0.2% (4/1854) of patients, including Grade 2 (0.1%) adverse reactions. Hyperthyroidism occurred in 0.4% (8/1854) of patients, including Grade 2 (0.3%) adverse reactions. Systemic corticosteroids were required in 25% (2/8) of patients with hyperthyroidism. Hypothyroidism occurred in 5% (97/1854) of patients, including Grade 3 (0.2%) and Grade 2 (3.6%) adverse reactions. Systemic corticosteroids were required in 6% (6/97) of patients with hypothyroidism.
BAVENCIO can cause immune-mediated type I diabetes mellitus, which can present with diabetic ketoacidosis. Monitor patients for hyperglycemia or other signs and symptoms of diabetes. Initiate treatment with insulin as clinically indicated. Withhold BAVENCIO for Grade 3 or Grade 4 endocrinopathies until clinically stable or permanently discontinue depending on severity. Immune-mediated type I diabetes mellitus occurred in 0.2% (3/1854) of patients, including Grade 3 (0.2%) adverse reactions.
BAVENCIO can cause immune-mediated nephritis with renal dysfunction. Withhold BAVENCIO for Grade 2 or Grade 3, and permanently discontinue for Grade 4 increased blood creatinine. Immune-mediated nephritis with renal dysfunction occurred in 0.1% (2/1854) of patients, including Grade 3 (0.1%) and Grade 2 (0.1%) adverse reactions. Systemic corticosteroids were required in all (2/2) patients with nephritis with renal dysfunction.
BAVENCIO can cause immune-mediated dermatologic adverse reactions, including rash or dermatitis. Exfoliative dermatitis including Stevens Johnson Syndrome (SJS), drug rash with eosinophilia and systemic symptoms (DRESS), and toxic epidermal necrolysis (TEN), has occurred with PD-1/PD-L1 blocking antibodies. Topical emollients and/or topical corticosteroids may be adequate to treat mild to moderate non-exfoliative rashes. Withhold BAVENCIO for suspected and permanently discontinue for confirmed SJS, TEN, or DRESS. Immune-mediated dermatologic adverse reactions occurred in 6% (108/1854) of patients, including Grade 3 (0.1%) and Grade 2 (1.9%) adverse reactions. Systemic corticosteroids were required in 25% (27/108) of patients with dermatologic adverse reactions.
BAVENCIO can result in other immune-mediated adverse reactions. Other clinically significant immune-mediated adverse reactions occurred at an incidence of <1% in patients who received BAVENCIO or were reported with the use of other PD-1/PD-L1 blocking antibodies. For myocarditis, permanently discontinue BAVENCIO for Grade 2, Grade 3, or Grade 4. For neurological toxicities, withhold BAVENCIO for Grade 2 and permanently discontinue for Grade 3 or Grade 4.
BAVENCIO can cause severe or life-threatening infusion-related reactions. Premedicate patients with an antihistamine and acetaminophen prior to the first 4 infusions and for subsequent infusions based upon clinical judgment and presence/severity of prior infusion reactions. Monitor patients for signs and symptoms of infusion-related reactions, including pyrexia, chills, flushing, hypotension, dyspnea, wheezing, back pain, abdominal pain, and urticaria. Interrupt or slow the rate of infusion for Grade 1 or Grade 2 infusion-related reactions. Permanently discontinue BAVENCIO for Grade 3 or Grade 4 infusion-related reactions. Infusion-related reactions occurred in 26% of patients, including three (0.2%) Grade 4 and ten (0.5%) Grade 3 infusion-related reactions. Eleven (85%) of the 13 patients with Grade ≥3 reactions were treated with intravenous corticosteroids.
Fatal and other serious complications of allogeneic hematopoietic stem cell transplantation (HSCT) can occur in patients who receive HSCT before or after being treated with a PD-1/PD-L1 blocking antibody. Follow patients closely for evidence of transplant-related complications and intervene promptly. Consider the benefit versus risks of treatment with a PD-1/PD-L1 blocking antibody prior to or after an allogeneic HSCT.
BAVENCIO can cause fetal harm when administered to a pregnant woman. Advise patients of the potential risk to a fetus including the risk of fetal death. Advise females of childbearing potential to use effective contraception during treatment with BAVENCIO and for at least 1 month after the last dose of BAVENCIO. It is not known whether BAVENCIO is excreted in human milk. Advise a lactating woman not to breastfeed during treatment and for at least 1 month after the last dose of BAVENCIO due to the potential for serious adverse reactions in breastfed infants.
A fatal adverse reaction (sepsis) occurred in one (0.3%) patient with locally advanced or metastatic urothelial carcinoma (UC) receiving BAVENCIO + best supportive care (BSC) as first-line maintenance treatment. In patients with previously treated locally advanced or metastatic UC, fourteen patients (6%) who were treated with BAVENCIO experienced either pneumonitis, respiratory failure, sepsis/urosepsis, cerebrovascular accident, or gastrointestinal adverse events, which led to death.
The most common adverse reactions (all grades, ≥20%) in patients with locally advanced or metastatic UC receiving BAVENCIO + BSC (vs BSC alone) as first-line maintenance treatment were fatigue (35% vs 13%), musculoskeletal pain (24% vs 15%), urinary tract infection (20% vs 11%), and rash (20% vs 2.3%). In patients with previously treated locally advanced or metastatic UC receiving BAVENCIO, the most common adverse reactions (all grades, ≥20%) were fatigue, infusion-related reaction, musculoskeletal pain, nausea, decreased appetite, and urinary tract infection.
Selected laboratory abnormalities worsening from baseline (all grades, ≥20%) in patients with locally advanced or metastatic UC receiving BAVENCIO + BSC (vs BSC alone) as first-line maintenance treatment were blood triglycerides increased (34% vs 28%), alkaline phosphatase increased (30% vs 20%), blood sodium decreased (28% vs 20%), lipase increased (25% vs 16%), aspartate aminotransferase (AST) increased (24% vs 12%), blood potassium increased (24% vs 16%), alanine aminotransferase (ALT) increased (24% vs 12%), blood cholesterol increased (22% vs 16%), serum amylase increased (21% vs 12%), hemoglobin decreased (28% vs 18%), and white blood cell decreased (20% vs 10%).
Please see full Prescribing Information and Medication Guide.
INDICATIONS
BAVENCIO® (avelumab) is indicated for:
- The maintenance treatment of patients with locally advanced or metastatic urothelial carcinoma (UC) that has not progressed with first-line platinum-containing chemotherapy
- The treatment of patients with locally advanced or metastatic UC who have disease progression during or following platinum-containing chemotherapy or have disease progression within 12 months of neoadjuvant or adjuvant treatment with platinum-containing chemotherapy
©2025 Merck KGaA, Darmstadt, Germany or its affiliates. All rights reserved. EMD Serono is the Healthcare business of Merck KGaA, Darmstadt, Germany in the U.S. and Canada. BAVENCIO and CoverOne are registered trademarks of Merck KGaA, Darmstadt, Germany or its affiliates.
US-AVE-01769 09/25
US-AVE-01769 09/25
This site contains medical information that is intended for residents of the United States only and is not meant to substitute for the advice provided by a medical professional. Always consult a physician if you have health concerns. Use and access of this site is subject to the terms and conditions as set out in our Legal Statement and Privacy Policy. This site contains information that is intended for US healthcare professionals only and governed by U.S. laws and government regulations. Canadian residents should consult the EMD Serono Canada Inc. website at www.emdserono.ca for information on products and services approved in Canada.
©2025 Merck KGaA, Darmstadt, Germany or its affiliates. All rights reserved.
EMD Serono is the Healthcare business of Merck KGaA, Darmstadt, Germany in the U.S. and Canada. BAVENCIO and CoverOne are registered trademarks of Merck KGaA, Darmstadt, Germany or its affiliates.
US-AVE-01769 09/25
US-AVE-01769 09/25
This site contains medical information that is intended for residents of the United States only and is not meant to substitute for the advice provided by a medical professional. Always consult a physician if you have health concerns. Use and access of this site is subject to the terms and conditions as set out in our Legal Statement and Privacy Policy. This site contains information that is intended for US residents only. Canadian residents should consult the EMD Serono Canada Inc. website at www.emdserono.ca for information on products and services approved in Canada.